Parents who seek support at my practice in Richmond do not usually arrive with a theoretical question. They arrive exhausted. They have been through the tantrums, the school refusals, the long silences, the headaches that come and go without explanation. They have often already tried the feelings charts, the reward systems, the breathing exercises. Some have received a diagnosis. Others are still waiting for one.
What most of them share is the sense that something important is not being reached.
This article draws on psychoanalytic thinking to offer a different frame for understanding emotional dysregulation in young people. Its central claim is not complicated: behaviour, particularly distressed behaviour, is never simply a malfunction. It is a communication. And what distinguishes psychoanalytic work from other approaches is the sustained commitment to hearing what that communication might be, rather than suppressing or correcting it.
Acting Out and Acting In: Two Structures of Distress
Psychoanalysis has long distinguished between two broad ways in which distress makes itself known. These are not personality types or diagnostic categories. They are structural tendencies — ways in which internal experience that cannot be expressed in words nevertheless finds a form.
The first is acting out. In psychoanalytic usage, acting out is not synonymous with misbehaviour, though it often looks that way from the outside. To act out is to stage something — to put into scene what cannot yet be put into speech. The explosive meltdown, the overturned chair, the defiance that seems wildly disproportionate to the immediate situation: these are enactments of an internal state that has no other available outlet. The child cannot say ‘I am overwhelmed by the sensory and social demands of my school environment and I feel fundamentally misunderstood,’ so they throw something instead. The action is addressed to an Other. It says: look at this. Notice that something is intolerable here.
Lacan’s seminar on anxiety is particularly useful here. He distinguishes acting out from the passage à l’acte (the passage to the act), and situates acting out as a fundamentally communicative gesture — one that remains, however chaotically, in the register of address. Something is being shown, if not said (Lacan, Seminar X, 1962–63).
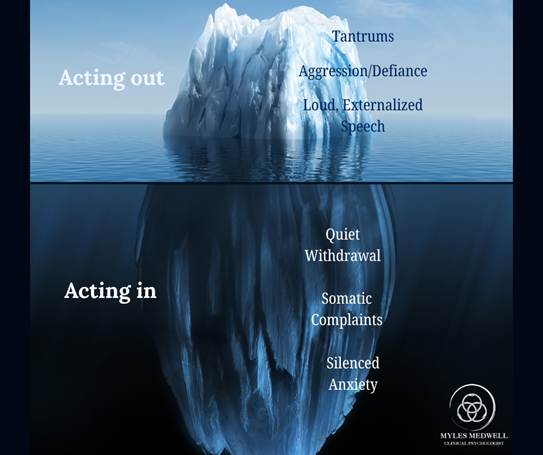
The second structure is acting in. Where acting out moves outward, acting in moves inward. These are the young people who do not cause disruption in the classroom and are therefore frequently missed. They withdraw, become very still, develop somatic complaints — the stomach aches that come every Sunday night, the headaches before assessments, the inexplicable fatigue. In adolescents, acting in often takes the specific form of masking: the exhausting performance of neurotypicality across the school day, followed by collapse once the safety of home permits it. Because they are not disruptive, their distress frequently goes unrecognised until it reaches crisis point.
Neither of these structures is preferable to the other. Both are attempts to manage something that cannot yet be borne otherwise. Both, from a psychoanalytic perspective, are worthy of attention rather than suppression.
Behaviour as Speech: A Psychoanalytic Orientation
Freud’s earliest work on hysteria established something that remains foundational to psychoanalytic thinking: that symptoms speak. The bodily conversion that Freud and Breuer documented in the 1890s – paralyses, anaesthesias, disturbances of vision and speech that had no neurological cause – were understood not as arbitrary malfunctions but as expressions. They said something. Often something that could not be said directly (Breuer and Freud, 1895).
This orientation applies equally to the behavioural symptoms of children and adolescents. A meltdown at precisely the same time each afternoon is not random. A refusal to enter a particular classroom is not simply defiance. The somatic complaint that appears on school mornings and resolves on weekends is not feigning. Each of these has a logic. The task of the clinician – and, often, the task of the parent – is to develop enough curiosity about that logic to begin to hear it.
Winnicott’s formulation is relevant here. In his paper ‘Communicating and Not Communicating Leading to a Study of Certain Opposites’ (1963), he proposes that there is a part of the self that never communicates and must not be disturbed. But he also observes that the failure to find a medium for communication – a space in which something can begin to be said – produces its own pathology. Behaviour, in this frame, is often the medium of last resort. It is what the subject resorts to when words have not been available, when words have not felt safe, or when what needs to be expressed exceeds the vocabulary of conscious speech.
Beyond the Diagnostic Frame
It is worth being clear about what this argument is not. It is not a claim that neurological difference is irrelevant, or that diagnoses like ADHD and autism spectrum disorder are without validity. They describe genuine and significant differences in how the nervous system is organised, and for many young people and families, a diagnostic framework provides important orientation.
The concern is with what happens when the diagnosis becomes the entire explanation. When a child’s distress is attributed entirely to a neurological deficit, the question of what the distress means for this particular child, at this particular moment, in this particular family and school context, can disappear. The individual subject is replaced by a category.
Psychoanalysis insists on the singularity of the subject. It asks not what disorder this child has, but what this child’s behaviour is saying, and to whom. As Plastow argues in his account of childhood and psychoanalytic discourse, the child is not reducible to their symptoms, and treatment that proceeds as though they are tends to address the surface while leaving the underlying structure untouched (Plastow, 2018).
This matters practically. A young person who has been told that their explosive behaviour is simply a consequence of their ADHD may internalise a position of helplessness with respect to it. They are not an agent in relation to their own distress; they are its victim. A psychoanalytic orientation, by contrast, treats the young person as a subject who is attempting something with their behaviour – even if what they are attempting has not yet become legible to anyone, including themselves.
Why Skill-Based Emotional Regulation Often Has Limits
The proliferation of emotional regulation resources in schools, clinics, and parenting programmes reflects a genuine effort to help. Zones of Regulation, breathing exercises, feelings identification cards, sensory tools: these are not without value, and for some young people in some contexts, they make a meaningful difference.
The limitation emerges most clearly at the moment they are most needed. During an acute meltdown, a neurodivergent collapse, or a somatic crisis, the young person is not in a position to consult a feelings chart. The cognitive and metacognitive capacities that skills-based approaches rely on are precisely the capacities that become unavailable under conditions of extreme affective arousal. What the child needs in that moment is not a tool. They need a regulated other, and they need a context in which what is happening makes some kind of sense.
This is not a criticism of the practitioners who deploy these approaches. It is an observation about the limits of any intervention that remains primarily at the level of conscious, deliberate self-management. Psychoanalytic work operates elsewhere – at the level of what is unconscious, structural, and repeated. It does not offer the young person a tool to manage their distress. It offers them a space in which the distress can begin to be spoken, and in being spoken, gradually transformed.
The research on treatment duration and outcomes is relevant here. Abbass and colleagues’ meta-analysis of intensive short-term dynamic psychotherapy in children and adolescents found significant effects on somatic symptoms, anxiety, and depressive symptoms, with gains maintained at follow-up (Abbass et al., 2013). Midgley and Kennedy’s systematic review of psychodynamic psychotherapy for children found promising outcomes across a range of presentations, with the quality of the therapeutic relationship consistently emerging as a central factor (Midgley and Kennedy, 2011).
Masking and the Cost of Performing Neurotypicality
The concept of masking has entered broader cultural awareness in recent years, partly through the advocacy and writing of autistic adults who have named and described their own experience. It refers to the sustained effort required to suppress, camouflage, or compensate for one’s neurodivergent traits in order to appear more neurotypical in social and academic settings.
The psychic cost of masking is significant and often severely underestimated by the adults in a young person’s life. A child who presents as calm and cooperative throughout the school day may be devoting enormous resources to maintaining that appearance. When they arrive home and collapse, become explosive, or shut down entirely, they are not being difficult. They are releasing the sustained tension of a performance that has occupied them for hours.

From a psychoanalytic perspective, masking is a particularly interesting formation. It involves the young person taking up a position in relation to the Other’s gaze – presenting what they believe is required of them, suppressing what they believe would be rejected. The relationship between the masked self and the subject’s actual experience becomes increasingly complex over time. In some adolescents, long-term masking produces a profound dissociation from their own desires, preferences, and modes of being – a loss of access to what Winnicott might call the true self (Winnicott, 1960).
Therapeutic work with masking adolescents requires, above all, a space in which the performance is not demanded. A consistent experience of being heard without being assessed, judged, or advised is, for many of these young people, genuinely novel.
What the Analytic Frame Offers
A psychoanalytic approach to working with young people does not proceed from a fixed curriculum or a predetermined outcome. It begins, as Lacan insists, from a position of not-knowing – a suspension of the assumption that the clinician already understands what the young person’s difficulty is about. This is more difficult than it sounds, particularly when a child arrives with an established diagnosis and a file of prior assessments.
The frame itself matters. Regular sessions, consistency, confidentiality, and a non-directive listening position are not peripheral features of the work. For a young person whose experience has been characterised by intrusion, misrecognition, or the relentless demand to be otherwise, the analytic frame may offer the first sustained encounter with a space that makes no demands.
Many adolescents arrive having already been explained to themselves. They have been told what their diagnosis means, what their behaviours indicate, what strategies they should be using. Psychoanalytic work inverts this. Rather than explaining the young person to themselves, it creates the conditions under which the young person can begin to speak about their own experience in their own terms. The difference is not merely procedural. It is, for many, the difference between an experience that confirms their sense of being known in advance and one that opens a genuine encounter with their own subjectivity.
A Note on Working with Parents
The young person’s distress does not exist in isolation. It arises within a relational context, and that context includes parents who are themselves often struggling, frightened, and exhausted.
A psychoanalytic orientation takes the parental experience seriously without making parents responsible for the child’s difficulty in a reductive way. Parents’ own histories, their relationship to their own adolescence, the unconscious material that a child’s behaviour stirs in them — these are not irrelevant. They are part of the field in which the young person’s distress is organised and responded to.
Parent consultations, separate from the young person’s own work, can provide a space to think about this material without it collapsing into advice or management. Sometimes the most useful thing a parent can do is not intervene differently, but understand something differently. That shift in understanding often produces a change in the relational field that the young person can feel, even if it is never directly spoken about.
At Myles Medwell Psychology in Richmond, I work with adolescents and young adults from approximately thirteen years of age, as well as with the parents and families who support them. Sessions are available in person at 53 Erin Street, Richmond, and via Telehealth across Victoria. Medicare rebates are available with a Mental Health Care Plan from your GP. A free fifteen-minute phone consultation is available for anyone wanting to explore whether this approach might be useful for their situation.
The first step is not to find the right technique. It is to find a space in which something can begin to be said.
References
Abbass, Allan A., Joanna Rabung, Joel Town, and others. ‘Short-Term Psychodynamic Psychotherapy for Children and Adolescents: A Systematic Review and Meta-Analysis.’ Journal of the American Academy of Child & Adolescent Psychiatry. 52, no. 8 (2013): 863–875.
Breuer, Josef, and Sigmund Freud. ‘Studies on Hysteria.’ Standard Edition of the Complete Psychological Works of Sigmund Freud, Vol. 2.. London: Hogarth Press, 1955. (Original work published 1895.)
Freud, Sigmund. ‘Remembering, Repeating and Working-Through. (1914.)’ The Standard Edition of the Complete Psychological Works of Sigmund Freud, Vol. 12.. London: Hogarth Press, 1958.
Lacan, Jacques. ‘The Seminar of Jacques Lacan, Book X: Anxiety, 1962–63.’ Translated by A. R. Price.. Cambridge: Polity Press, 2014.
Lacan, Jacques. ‘The Seminar of Jacques Lacan, Book XI: The Four Fundamental Concepts of Psychoanalysis.’ Translated by Alan Sheridan.. New York: Norton, 1981.
Midgley, Nick, and Irene Kennedy. ‘‘Psychodynamic Psychotherapy for Children and Adolescents: A Critical Review of the Evidence Base.’’ Journal of Child Psychotherapy. 37, no. 3 (2011): 232–260.
Plastow, Michael. ‘What Is a Child? Childhood, Psychoanalysis, and Discourse.’ London: Karnac, 2018.
Winnicott, D. W. ‘‘Communicating and Not Communicating Leading to a Study of Certain Opposites.’ (1963.)’ The Maturational Processes and the Facilitating Environment.. London: Hogarth Press, 1965.
Winnicott, D. W. ‘‘Ego Distortion in Terms of True and False Self.’ (1960.)’ The Maturational Processes and the Facilitating Environment.. London: Hogarth Press, 1965.
Winnicott, D. W. ‘Playing and Reality.’ London: Tavistock, 1971.