Most people considering psychological treatment do not spend much time wondering which theoretical tradition underpins their therapist’s approach. They want to feel less anxious, less stuck, less at the mercy of patterns they cannot quite name. They want to understand why they keep arriving at the same impasses.
That is a reasonable starting point. But it raises a question that is worth taking seriously: which kind of therapy is likely to help, and why?
Psychoanalytic therapy occupies a particular place in this landscape. It is not a brief intervention. It is not primarily concerned with symptom reduction, skill-building, or the correction of unhelpful thoughts. Its focus is on the unconscious, on the structure of the subject’s suffering, on what is being said, avoided, repeated, and not yet put into words.
For the right person, this distinction matters enormously.
What Psychoanalytic Therapy Is
Psychoanalytic therapy is a form of talk therapy rooted in the tradition established by Sigmund Freud in the late nineteenth century and developed by successive thinkers which includes Klein, Winnicott, Bion, and, in a particularly radical direction, Jacques Lacan.
At its foundation is a specific claim: that much of human suffering is not simply conscious and accessible, but is shaped by processes operating outside of awareness – the unconscious. These processes are not simply ‘repressed memories’ in the popular sense. They are structural features of how the subject is organised in relation to language, desire, the body, and the Other.
What follows from this claim is a particular way of working. Rather than targeting symptoms directly through techniques, strategies, or structured exercises, psychoanalytic therapy creates space for the subject’s own speech to unfold. It proceeds through free association. This is the invitation to say whatever comes to mind, without censorship. It pays careful attention not only to what is said, but to how it is said: to repetitions, contradictions, slips, hesitations, dreams, and silences.
The aim is not comfort. The aim is truth. A truth that is discovered through the analytic process rather than delivered in advance.
Freud’s foundational papers on technique remain relevant here. His account of the unconscious, resistance, transference, and the fundamental rule of free association established the architecture of psychoanalytic work that all subsequent traditions, however they differ, continue to inhabit (Freud, 1912, 1913, 1914).
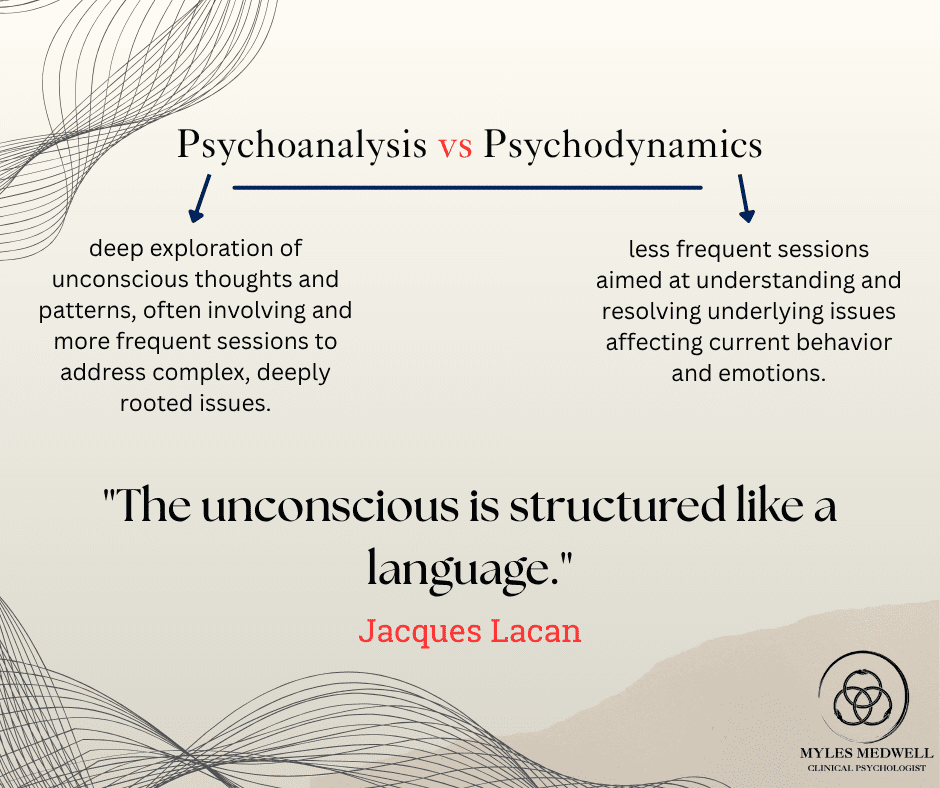
Psychoanalytic Versus Psychodynamic Therapy: A Useful Distinction
The terms are often used interchangeably, and the distinction is not always observed carefully in clinical settings. But it is worth making.
Psychodynamic therapy is a broader category that draws on psychoanalytic ideas particularly the importance of the unconscious, early relationships, and the therapeutic relationship. This kind of therapy applies these ideas in more structured, shorter-term formats. It tends to be integrative, goal-directed, and relatively accessible within standard health settings.
Psychoanalytic therapy refers more specifically to approaches that remain committed to the core features of the analytic frame: free association, the sustained exploration of the unconscious, attention to transference, and a willingness to tolerate open-endedness rather than imposing direction from outside.
This distinction has some empirical grounding. Shedler’s influential review of the evidence for psychodynamic psychotherapy found that the effects of psychodynamic treatment are comparable to those reported for other therapies, and that they tend to continue to improve after treatment ends. This pattern is rarely observed in briefer, more structured approaches (Shedler, 2010). More recently, Driessen and colleagues found that long-term psychoanalytic therapy produced significantly larger effects than short-term forms for complex presentations (Driessen et al., 2015).
In other words: depth tends to take time. This is not a limitation. It is a structural feature of what depth-oriented work involves.
The Lacanian Approach: Language, the Unconscious, and the Subject
Jacques Lacan was a French psychoanalyst who undertook a sustained, rigorous, and in many respects radical re-reading of Freud from the 1950s onward. His influence on psychoanalytic practice, particularly in France, Latin America, and Australia, has been significant.
Lacan’s central proposition – that the unconscious is structured like a language – is both precise and far-reaching in its implications. It does not mean that the unconscious communicates through words in the ordinary sense. It means that the unconscious operates according to the same logic as language: through substitution, displacement, condensation, and the sliding of meaning beneath apparently fixed signifiers.
In practice, this shifts the analyst’s attention. A Lacanian analyst listens not only to the content of what is said, but to the signifiers themselves: the particular words and phrases the subject returns to, the places where speech breaks down, the points where something seems to resist articulation, the gaps between what is intended and what arrives.
The analyst’s role, in this frame, is not to be an expert on the subject’s life. It is not to offer insight, advice, or a corrective emotional experience. It is to hold a position of ‘not-knowing’ that makes it possible for the subject’s own unconscious knowledge to emerge or to appear, as Lacan put it, in the cracks of what is said.
The Freudian School of Melbourne (formerly the Melbourne School of Freudian Studies) continues to develop and teach this approach in Australia, maintaining close ties to international Lacanian networks and training. This is the tradition in which my work is grounded.
What Actually Happens in a Session
This is the question most people do not quite know how to ask but most want answered.
A psychoanalytic session is relatively unstructured compared to most other forms of therapy. There is no worksheet, no agenda, no homework, no CBT triangle to complete. The guiding invitation is free association: to speak whatever comes to mind, to follow the movement of thought and feeling without editing, selecting, or organising it toward a conclusion.
This takes practice. Most people are not accustomed to speaking without an implicit audience in mind, without the expectation of being interrupted, corrected, or redirected. Learning to speak freely is itself part of the work.
The therapist listens. Occasionally they speak, sometimes to offer a reflection, to ask a question, to note something that seems significant. But the analyst does not fill silence with reassurance or respond to every disclosure with an interpretation. The pace is determined by what is emerging, not by an external protocol.
Sessions are typically fifty minutes in length and held weekly, though more frequent sessions are sometimes possible and clinically indicated. Both in-person appointments and telehealth are available at Myles Medwell Psychology in Richmond.
What Psychoanalytic Therapy Is Particularly Well-Suited To
Psychoanalytic and psychodynamic approaches have an evidence base across a range of presentations. They are particularly well-suited to experiences that feel complex, layered, or that have not responded to shorter-term interventions.
These include persistent anxiety and depression, particularly where the cause is not obvious or where symptoms return despite previous treatment. Complex and developmental trauma, where experience has not yet been fully articulated or where its effects continue to structure the present. Repetitive relational patterns, where the same dynamics arise across different contexts and relationships. Questions of identity, desire, sexuality, and belonging, where the difficulty is not a discrete symptom but a more pervasive sense of not quite knowing who one is or what one wants. Dissociation, functional neurological symptoms, and somatic presentations, where the body speaks what has not yet found its way into words. Personality disorders and other presentations that benefit from longer-term, depth-oriented work.
Town and colleagues conducted a meta-analytic review of intensive short-term dynamic psychotherapy and found significant effects across a range of symptom and interpersonal domains (Town et al., 2017). Leichsenring and colleagues’ review of psychoanalytic and psychodynamic therapies for personality disorders found substantial clinical benefit for long-term approaches with complex presentations (Leichsenring et al., 2015).
How It Differs from CBT
Cognitive Behavioural Therapy is the most commonly offered psychological treatment in Australia. It has a robust evidence base for anxiety and depression and produces meaningful short-term relief for many people.
But CBT and psychoanalytic therapy proceed from different assumptions and work toward different things.
CBT focuses on the relationship between thoughts, feelings, and behaviours. It is structured, goal-directed, and typically time-limited. Its aim is to identify and modify unhelpful thought patterns, build coping skills, and reduce symptoms.
Psychoanalytic therapy is less concerned with the content of cognitions and more concerned with their structure: where they come from, what function they serve, what they might be defending against, and what they leave unsaid. Rather than modifying a thought, psychoanalytic work asks why this thought, why now, and what it means for this particular person at this particular moment.
This is not a competition. Both approaches have their place. But for people who have found that symptom management didn’t hold, a psychoanalytic approach may offer something closer to what they are looking for.
There is also growing empirical support for this distinction. Fonagy’s Tavistock Depression Study found that long-term psychoanalytic therapy produced superior outcomes to shorter-term treatment at long-term follow-up, particularly for complex and chronic presentations (Fonagy et al., 2015). This matters: it is not that psychoanalytic therapy is slower; it is that its effects continue to deepen after the work is formally complete.
Is Psychoanalytic Therapy Right for You?
It tends to suit people who are curious about themselves; who are willing, at least provisionally, to entertain the possibility that the explanation for their difficulties might lie somewhere other than where they have been looking. It suits people who feel that something important has not yet been said, perhaps not even to themselves.
It tends to suit people who have tried briefer approaches and found them useful but insufficient. Who have understood their patterns without being able to change them. Who can say what is wrong without being able to say what it means.
It requires a willingness to tolerate uncertainty, to stay with what is difficult, and to engage in a process that does not always move in a straight line. It is not a quick fix. But for people for whom quick fixes have not fixed much, this may be exactly the point.
The question of fit is always individual. A free fifteen-minute phone consultation is available to anyone who wants to explore whether this approach makes sense for their particular situation. There is no obligation.
Practical Information
As a registered Clinical Psychologist, my practice accept Medicare rebates under a Mental Health Care Plan, which can be obtained from your GP in a single appointment. NDIS funding and TAC referrals are also accepted. A sliding-scale fee structure is available.
The standard session fee is $245 for a fifty-minute appointment, below the Australian Psychological Society’s recommended rate for clinical psychologists. Sessions are available in person at 53 Erin Street, Richmond, Melbourne, and via telehealth across Victoria and Australia-wide.
If something here has resonated, or if you simply want to understand more before deciding, you are encouraged to reach out.

About Myles Medwell
Myles Medwell is a Clinical Psychologist based in Richmond, Melbourne, specialising in Lacanian psychoanalytic and psychodynamic therapy. He holds a Master of Psychology (Clinical) from Federation University, is registered with AHPRA, and is a member of the Australian Clinical Psychology Association. He is currently undertaking ongoing training at the Freudian School of Melbourne.
He works with adolescents and adults across a wide range of presentations, including complex trauma, dissociation, Functional Neurological Disorder, personality disorders, anxiety, depression, and identity-related concerns. Comprehensive psychological assessments are also available. GP, psychiatrist, and allied health referrals are welcome.
53 Erin Street, Richmond Melbourne VIC | www.mylesmedwell.com.au | Free 15-minute phone consultation available via the website.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR. 5th ed., text rev. Washington, DC: American Psychiatric Association Publishing, 2022.
Driessen, Ellen, Jacques J. D. M. van Hemert, Cuijpers, Pim, Hollon, Steven D., and others. “Long-term Efficacy of Psychoanalytic Psychotherapy: A Systematic Review and Meta-Analysis.” Psychological Medicine 45, no. 5 (2015): 1069–1080.
Fonagy, Peter, Halina Rost, Jo-Anne Carlyle, Sally McPherson, Roger Thomas, R. D. Pasco Fearon, David Goldberg, and Nick Taylor. “Pragmatic Randomized Controlled Trial of Long-Term Psychoanalytic Psychotherapy for Treatment-Resistant Depression.” World Psychiatry 14, no. 3 (2015): 312–321.
Freud, Sigmund. “Recommendations to Physicians Practising Psycho-Analysis.” 1912. In The Standard Edition of the Complete Psychological Works of Sigmund Freud, Vol. 12. London: Hogarth Press, 1958.
Freud, Sigmund. “On Beginning the Treatment.” 1913. In The Standard Edition of the Complete Psychological Works of Sigmund Freud, Vol. 12. London: Hogarth Press, 1958.
Freud, Sigmund. “Remembering, Repeating and Working-Through.” 1914. In The Standard Edition of the Complete Psychological Works of Sigmund Freud, Vol. 12. London: Hogarth Press, 1958.
Lacan, Jacques. The Seminar of Jacques Lacan, Book XI: The Four Fundamental Concepts of Psychoanalysis. Translated by Alan Sheridan. New York: Norton, 1981.
Lacan, Jacques. “The Function and Field of Speech and Language in Psychoanalysis.” 1953. In Écrits: A Selection. Translated by Alan Sheridan. London: Tavistock, 1977.
Leichsenring, Falk, Sven Rabung, and Eric Leibing. “The Efficacy of Short-Term Psychodynamic Psychotherapy in Specific Psychiatric Disorders: A Meta-Analysis.” Archives of General Psychiatry 61 (2004): 1208–1216.
Leichsenring, Falk, Frank Leweke, Gerhard Rudolf, and Christoph Mundt. “The Empirical Status of Psychodynamic Psychotherapy: An Update.” Psychotherapy and Psychosomatics 84, no. 3 (2015): 129–148.
Shedler, Jonathan. “The Efficacy of Psychodynamic Psychotherapy.” American Psychologist 65, no. 2 (2010): 98–109.
Town, Joel M., Allan Abbass, Christoph Diener, Chiara De Rubeis, and others. “A Randomised Controlled Trial of Intensive Short-Term Dynamic Psychotherapy for Complicated Grief and Mourning.” Journal of Nervous and Mental Disease 205, no. 9 (2017): 690–698.